ann gifted me a privately guided walking tour of edinburgh for my birthday! there is an outsized history of medicine and medical discoveries in edinburgh, and it was very fascinating. the tour began at the greyfriars kirkyard, which is a ancient cemetery in the center of edinburgh. there, metal cage-like barriers would be placed over recent graves to prevent grave robbers from stealing recently deceased bodies, which they could sell as cadavers, which were in high and unregulated demand in the early days of formalized medical education.
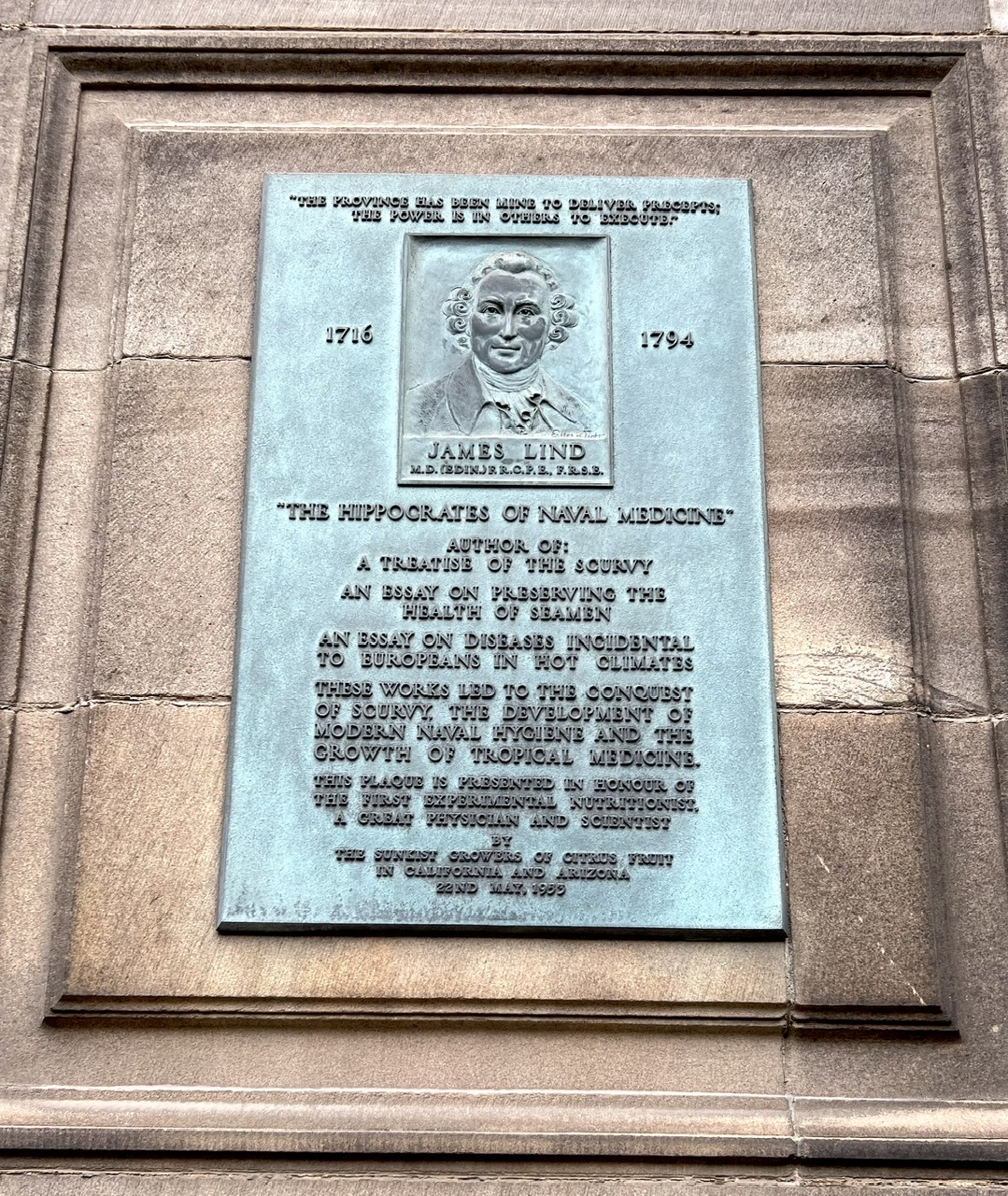
we then proceeded to mcewan hall, the home of the medical school at the university of edinburgh. many important medical discoveries were made in edinburgh, including the etiology of scurvy by james lind, and many others.
the next stop was the meadows, a large open area of grass on the campus of the university of edinburgh. beneath the meadows are thousands of unmarked graves, as this was were bodies were buried during the bubonic plague. reportedly, occasionally students and tourists relaxing on the grass still find pieces of human bones sifting up from beneath the earth.
another stop was the surgeon hall museums, the first anatomy and pathology museum in the world. this is also where there was a riot in 1870 in support of the “edinburgh seven,” seven women who agitated for the right to study medicine at the medical school when women were not allowed to do so. unfortunately, it took an inordinate amount of time even after these riots for the medical schools to begin to allow women to matriculate.
we also went to the old surgeon’s hall at the university of edinburgh, which was a cadaver lab in the early days of formal medical education. private cadaver labs were started as educational competition/supplementation to the medical school, and to supply cadavers, they would need to be purchased, often under questionable circumstances, such as being snatched from recent graves. robert knox ran one of the most well known cadaver labs, where he would dissect the freshest cadavers for the education of medical students. at least 16 of these bodies were procured from william burke and william hare, who had murdered their victims for this purpose. we also walked by the medical lecture hall of joseph lawrence, the father of modern surgical sterilization, the inventor of listerine, and the founder of the johnson and johnson company.
the tour ended at the old college of the university of edinburgh, where there is a nondescript plaque in honor of one the british military’s most famous surgeons for decades of the 1800s, james barry, who served all over the world and tremendously improved sanitation standards. the fascinating thing about james barry was that they were actually a woman, whose real name was margaret ann bulkley, a fact not realized by anyone else until after her death. it was an era in which women were not permitted to practice medicine. the plaque and all the military records still read “james barry.”